Background: We highlight a case series of two symptomatically similar patients representing vastly different aetiologies of pancytopenia. Pancytopaenia can be categorized by its pathological cause – as a result of: decreased production (e.g. autoimmune disorders, HLH, nutritional deficiency, aplastic anaemia, drugs, chemotoxic agents, as well as juvenile pernicious anaemia and also viral infections, increased destruction (DIC, infections, Rheumatoid Arthritis or bone marrow infiltration (leukaemia. It can also be categorized grossly by malignant versus non-malignant causes. Prevalence of causes and appropriate investigations are paramount to a timely, accurate diagnosis.
Case presentation: This case report was completed through retrospective chart analysis.
Results: Case 1: A previously well-term baby boy of 5 months, presenting with lethargy and poor feeding. Baby boy (BB) on initial blood work had a megaloblastic anaemia, pancytopenia and accompanying motor and social developmental delay. He also had a poor swallow, aspirating on liquids. Investigations showed that BB was severely B12 deficient due to maternal deficiency, as he was solely breastfed, with no alternate diagnosis found. MRI brain showed no demyelination. BB was treated with B12 injections to become replete, and while he has improved developmentally, he still does not have a safe swallow.
Case 2: A previously well-term baby girl of 2 months, presenting with lethargy and poor feeding. On basic bloods, like the baby boy, Baby Girl(BG), had a pancytopenia, however she also had a microcytic anaemia with a significant transaminitis. Unfortunately, she quickly deteriorated, with her bloods concerning for HLH (later confirmed on bone marrow biopsy and genetic testing showing perforin deficiency), also requiring ventilator support for ARDS from HMPV infection. She was quickly initiated on methylprednisolone IVIG and cyclosporine to manage her condition. BG is improved and awaiting a haematopoietic stem cell transplant.
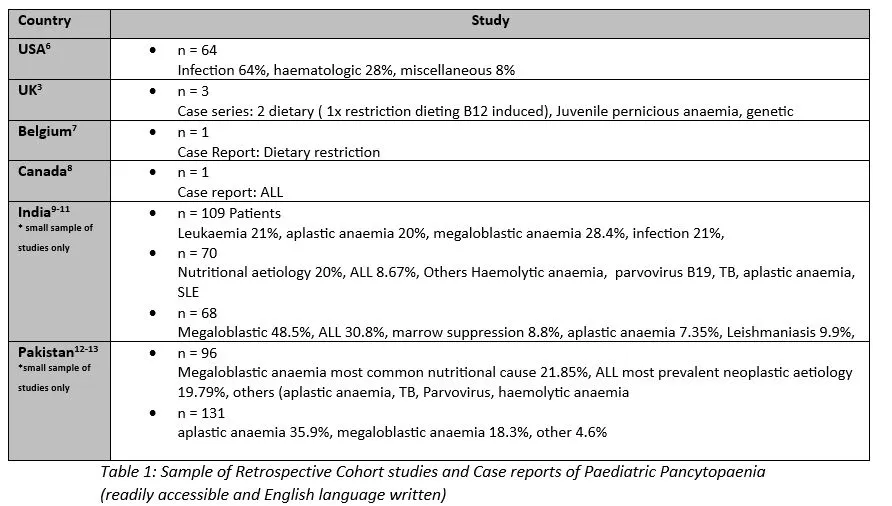
Discussion: From the current literature, there are few case reports and no comprehensive analysis of the prevalence of specific aetiologies in Western, English speaking countries (3,6–8, Table 1). In contrast, in countries such as India and Pakistan, many retrospective studies are published (highest prevalence: nutritional deficiency, leukaemia, aplastic anaemia), where ethnicity and nutrional status play a role in aetiology . We highlight our cases in Ireland to contribute to the data of aetiological prevalence in the Western English-speaking countries. Our case of B12 deficiency induced pancytopaenia – secondary to dietary deficiency, is more commonly described as being secondary to malnutrition in impoverished regions . However, here it has occurred as result of dietary preference. We note other similar cases where dietary restriction also led to pancytopaenia and B12 deficiency .
Learning points: As pancytopenia can have vastly different causes, a wide differential , should be considered to correctly diagnose patients. While some articles , book chapters, and case reports attempt to outline a framework, no guidelines exist with an investigative algorithm published in the USA, UK, Canadian, Australian, European or International Haematology journals/societies. This represents a gap in the literature and such a guideline with an investigative algorithm, formulated in conjunction with haematology colleagues, would greatly benefit the paediatric patient population.