Background: Acute asthma poses significant health burdens. Despite many standard guidelines, suboptimal management remained and has negative effect on the quality of care and outcomes.
Objective: To evaluate the impact of the institutional care guideline for acute asthma in hospitalized children, focusing on treatment outcomes and medical expenses.
Methods: This quality improvement retrospective cohort study involved children aged 1–15 years hospitalized due to acute asthma before and after the institutional acute asthma care guideline implementation during 2016–2024. The guideline consists of standard treatment protocol including stepwise use of bronchodilator and respiratory support as well as discharge planning. The guideline implemented using a Plan-Do-Study-Act (PDSA) cycle.
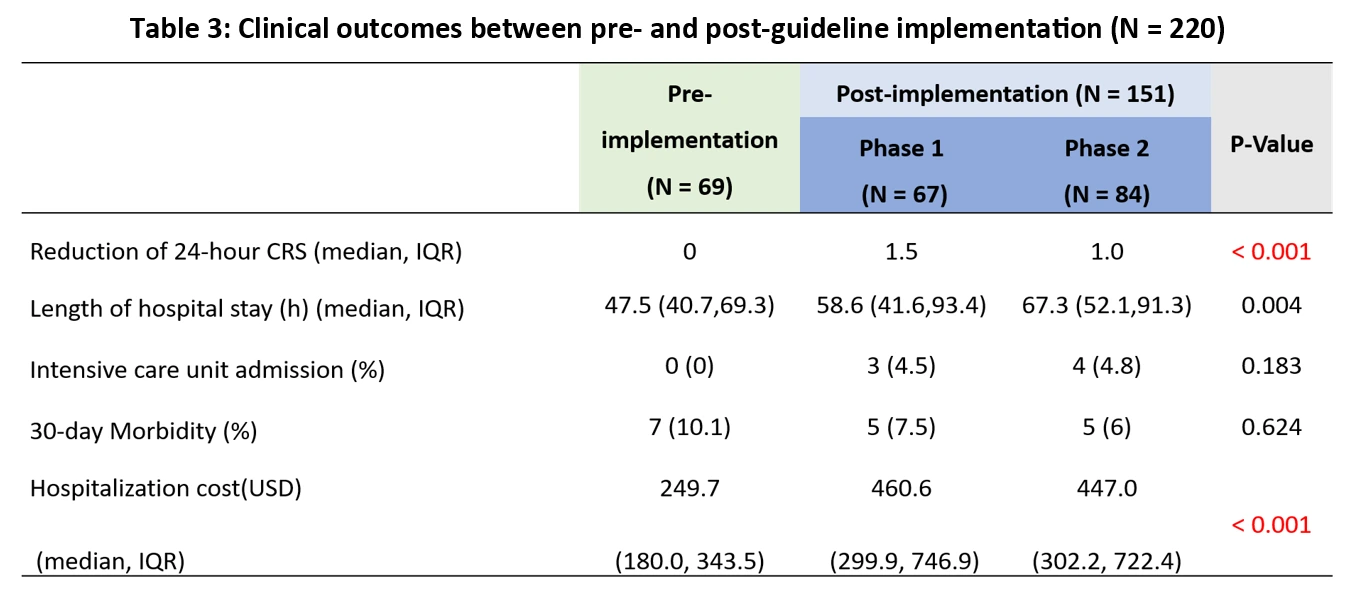
Results: A total of 220 hospitalized acute asthma children were reviewed (69 pre- and 151 post-implementation group). After guideline implementation, there is a significant reduction in time to first in-hospital bronchodilator (117 vs. 104 vs. 70 mins, p < 0.001), also a significant increase in use of nebulized steroids (0 vs 27 vs. 5, p < 0.01) and high flow nasal cannula (3 vs. 24 vs. 29, p < 0.001). For clinical outcomes, the 24-hour clinical respiratory score significantly improved after guideline implementation (1.06-point, p < 0.001). However, the increase in length of hospital stay (47.5 vs. 65.6 h, p = 0.003) and total medical expenses (249.7 vs. 460.6 vs. 447.0 USD, p < 0.001) were observed in the post-implementation group (Table 1).
Conclusion: The developed acute asthma care guideline for hospitalized children can improve clinical outcomes faster but cannot decrease hospital length of stay. The cost-effectiveness of the developed guideline required further evaluation.